This site is intended for United Kingdom/Ireland healthcare professionals
Decision-making factors in AML:
Insights from BSH 2022
Treatment selection and care for patients with AML can be challenging, so we spoke to three experts in the field about their practice and the factors they consider when making choices for, and with, their patients.

Explore the questions and watch the videos below to find out what drives decision-making for Dr Victoria Campbell, Dr Steven Knapper and Dr Priyanka Mehta
 Incorrect - 35%
Incorrect - 35%Patients received an HSCT in each study at the following rates:
France RWE: 35%1
England RWE: 25%2
Germany RWE: 62%3
Italy RWE: 40% of those who achieved CR/CRi4
Patients received an HSCT in each study at the following rates:
France RWE: 35%1
England RWE: 25%2
Germany RWE: 62%3
Italy RWE: 40% of those who achieved CR/CRi4
Incorrect - 16 months - NRFrance RWE: 16.1 months1
England RWE: 16.6 months2
Germany RWE: 21 months3
Italian RWE: mOS NR - 68.6% at 12 months4
France RWE: 16.1 months1
England RWE: 16.6 months2
Germany RWE: 21 months3
Italian RWE: mOS NR - 68.6% at 12 months4
Incorrect - Intensive anti-leukaemic therapy followed by post-remission therapyRecommendation 1
Anti-leukaemic therapy over best supportive care5
Recommendation 2
Intensive anti-leukaemic therapy over less-intensive anti-leukaemic therapy5
Recommendation 3
Patients who achieve remission following at least one cycle of intensive anti-leukaemic therapy should receive allogeneic HSCT if elligible. ASH guidelines suggest ineligible patients should receive postremission therapy over no additional therapy5
Recommendation 1
Anti-leukaemic therapy over best supportive care5
Recommendation 2
Intensive anti-leukaemic therapy over less-intensive anti-leukaemic therapy5
Recommendation 3
Patients who achieve remission following at least one cycle of intensive anti-leukaemic therapy should receive allogeneic HSCT if elligible. ASH guidelines suggest ineligible patients should receive postremission therapy over no additional therapy5
Incorrect - All of the aboveECOG PS, cytogenetic risk, comorbidities, and age are all among the factors to be considered in patient assessment and treatment selection7-9
ECOG PS, cytogenetic risk, comorbidities, and age are all among the factors to be considered in patient assessment and treatment selection7-9
Incorrect - 6-8 daysMedian time to platelet and neutrophil recovery is 6-8 days longer with Vyxeos Liposomal vs DA 3+76
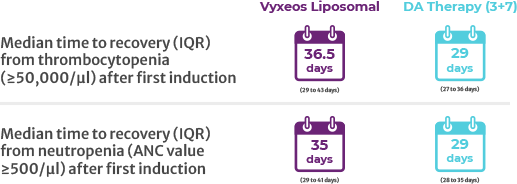
Median time to platelet and neutrophil recovery is 6-8 days longer with Vyxeos Liposomal vs DA 3+76
Incorrect - FalseDay 30 and Day 60 mortality rates were lower with Vyxeos Liposomal vs DA 3+7:
France RWE: 30-day – 6%, 60-day – 8%1
England RWE: 30-day – 7%, 60-day – 15%2
Germany RWE: 30-day – 8%3
Italian RWE: 60-day – 7%4
Study 301: Vyxeos Liposomal 30-day - 6%, 60-day - 14% vs DA 3+7 30-day - 11%, 60-day 21%6
Day 30 and Day 60 mortality rates were lower with Vyxeos Liposomal vs DA 3+7:
France RWE: 30-day – 6%, 60-day – 8%1
England RWE: 30-day – 7%, 60-day – 15%2
Germany RWE: 30-day – 8%3
Italian RWE: 60-day – 7%4
Study 301: Vyxeos Liposomal 30-day - 6%, 60-day - 14% vs DA 3+7 30-day - 11%, 60-day 21%6